Case: A helmeted 13-yo-boy carrying a friend on his e-scooter ran into a pole and was pinned against the handle. He was brought in by his parents for chest pain from periphery to SMH. His CXR shows rib fractures and a tension hemopneumothorax. He is hypoxic and requires a decompression. What is the ideal location for needle decompression according to 2025 ATLS?
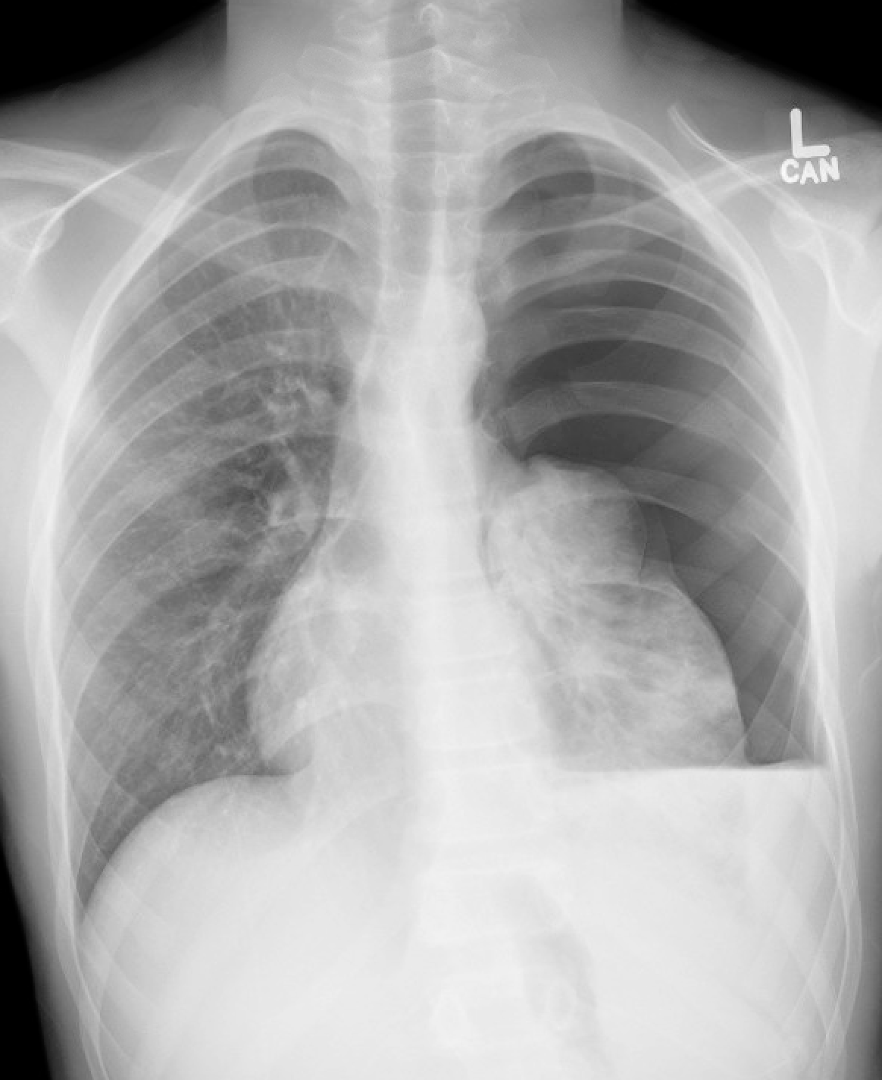
Discussion: 2025 ATLS recommends 2nd ICS at midclavicular line in peds and 4th/5th ICS anterior to midaxillary line in adults. Transition from peds to adult for placement site is considered based on chest wall thickness and patient size (around age 13). See latest EB article for a deeper dive.
